- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
Cite as: Archiv EuroMedica. 2026. 16; 1. DOI 10.35630/2026/16/Iss.1.019
Laryngectomy is a surgical intervention that involves the partial or complete excision of the larynx, which is the primary organ responsible for phonation and airway protection. The most common indications for laryngectomy are malignancies of the larynx or severe trauma resulting in extensive damage to the larynx. The surgical procedure can be performed as a partial laryngectomy, which involves the removal of a portion of the larynx, or as a total laryngectomy, which requires the complete removal of the larynx, including the vocal folds, hyoid bone, epiglottis, thyroid and cricoid cartilage, and several rings of tracheal cartilage. This surgical intervention results in the separation of the upper airway from the oral cavity, nasopharynx, and esophagus, requiring the establishment of an alternative means for respiration and speech production. The management of patients who undergo laryngectomy requires a multidisciplinary approach, including the involvement of speech therapist and psychologists, among other healthcare professionals, to optimize the rehabilitation process and improve patient outcomes.
A 66-year-old male patient with a 30-year history of cigarette smoking was admitted to the ear, nose, and throat (ENT) clinic for complaints of hoarseness and dysphagia that had been present for several months. On examination, the patient's throat was unchanged, and there was no purulent discharge from the nose. The patient was diagnosed with laryngeal carcinoma, stage T3N1M0.
Total laryngectomy is a highly effective treatment option for advanced stage laryngeal cancer, with 5-year survival rates ranging from 53% to 86%. Patients who undergo total laryngectomy and receive a voice prosthesis and voice rehabilitation with a speech therapist report better voice quality and overall quality of life, which can help to reduce the risk of depression and anxiety following surgery.
Keywords: Laryngectomy, laryngology, laryngeal cancer, voice rehabilitation, Speech therapy, Voice prosthesis, Phonosurgery, Swallowing rehabilitation
Malignant tumors affecting the larynx are the most common types of malignancies observed in the head and neck region. Following lung cancer, they represent the most prevalent respiratory tract cancers. In Poland, laryngeal cancer ranks as the seventh most common cancer among males, accounting for 3.4% of all cases. The incidence rate is higher in males, with a ratio of 10:1 compared to females, at 12.1/100,000 and 1.6/100,000, respectively. Laryngeal cancer typically manifests in individuals aged 40 to 60 years [1]. Squamous cell carcinoma represents the most common type of laryngeal malignancy, accounting for 95% of cases [2]. Risk factors associated with laryngeal cancer include smoking, alcohol consumption, and pre-cancerous conditions such as leukoplakia and laryngeal papillomas [3].
Laryngectomy is the standard treatment for laryngeal cancer, laryngeal fractures, trauma-induced larynx damage, and radiotherapy-related chondronecrosis. However, less invasive therapies such as radiotherapy and chemotherapy are preferred in many cases. Laryngectomy becomes necessary when these therapies fail to preserve the larynx or when the cancer has progressed beyond a stage that precludes normal function [4]. Diagnosis of laryngeal cancer involves a variety of imaging techniques, including computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET), as well as biopsy examination of the cancer tissue.
The TNM system is used to classify tumors, and increasing classifications from T1 to T4 indicate the extent of tumor spread, thereby informing the most appropriate treatment approach [5]. T1-T3 tumors are typically treated with radiotherapy, laser chordectomy, or partial laryngectomy, whereas T3-T4 tumors require total laryngectomy [6]. Total laryngectomy has a high 5-year survival rate (53-86%) for advanced-stage laryngeal cancer [7]. Following laryngectomy, the airway anatomy and physiology are altered, and patients breathe through a stoma created by the tracheostomy, resulting in a disconnection between the trachea and the mouth and nose. Rehabilitation following laryngectomy includes voice restoration and oral feeding [8].
The aim of this article is to present a clinical case of a patient with advanced laryngeal cancer treated by total laryngectomy with cervical lymph node dissection, followed by a description of the surgical approach and the stages of postoperative voice rehabilitation.
The choice of the case report format is justified by the need for a detailed presentation of an individual clinical observation in a patient with locally advanced laryngeal cancer staged as T3N1M0, which allows tracing the diagnostic pathway, the rationale for surgical treatment, the characteristics of the operative intervention, and subsequent restoration of breathing and speech functions. Presentation of a single case makes it possible to demonstrate the clinical course of the disease and the practical implementation of an oncological treatment strategy in real clinical practice.
The clinical context of this observation is associated with late presentation, a long history of tobacco use, and tumor extension to laryngeal structures and regional lymph nodes, which excluded organ preserving treatment options and determined the need for radical surgical intervention. A significant aspect of the clinical situation is the loss of natural voice following surgery and the necessity for comprehensive rehabilitation.
The article subsequently presents the clinical case of a patient with laryngeal cancer, provides a detailed description of diagnostic findings and the performed surgical procedure, and discusses postoperative management and voice rehabilitation using a tracheoesophageal voice prosthesis.
A 66-year-old male patient presented to the ENT clinic with chronic laryngitis (J37.0) characterized by hoarseness and dysphagia for several months. The patient has a 30-year history of smoking cigarettes. Upon ENT examination, the throat appeared unchanged and the nose was clear without purulent discharge. However, on indirect laryngoscopy, infiltration of the left vocal fold was observed.
To further evaluate the patient, a CT scan of the larynx was ordered with intravenous contrast agent [Figure 1.]. The CT scan revealed a pathological mass with disintegrative features measuring approximately 24 x 10 x 37 mm within the vestibular fold on the left side. The lower pole of the mass reached the subglottic region, and the upper pole of the mass abutted the fat body without any features of thyroid cartilage destruction. There were no signs of infiltration of the spoids.
In addition, a visibly enlarged lymph node of group IIB with destructive features was found on the left side, measuring approximately 12 x 16 mm in cross-section. Single lymph nodes of groups VA and VB were also present, measuring up to 5 mm in cross-section.
Numerous massive polyps were observed on the left side of the glottis.
![[Figure 1.]](artikel-19-bild-1.jpg)
[Figure 1.]
The patient was admitted to the ENT department for laryngeal microsurgery. Prior to the procedure, additional examinations were performed, and the patient was placed under general anesthesia. The excised tissue was sent for histopathological examination, and the patient was subsequently discharged from the ward in good general condition with a recommendation for follow-up in the ENT Outpatient Clinic.
The histopathological examination revealed G2 non-squamous squamous cell carcinoma, with immunohistochemical staining showing CK5/6+ and p63+, but negative for p16-. An H/P.1 rapid oncology therapy card was established based on these findings.
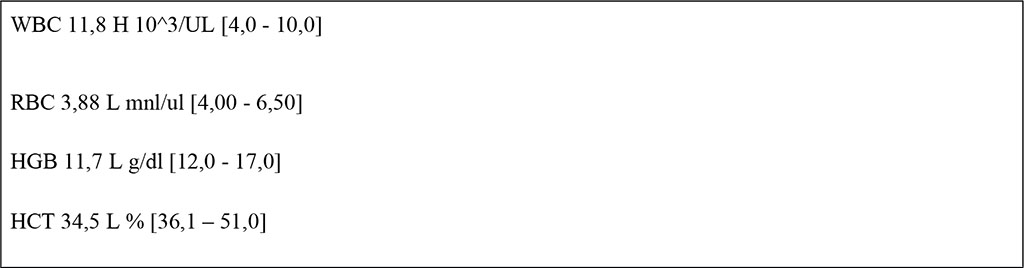
In addition, the patient's blood test results showed the following values:
The patient with laryngeal carcinoma was referred for surgical treatment (laryngectomy with lymphadenectomy) after oncological consultation. The diagnosis was C32.0 laryngeal carcinoma T3N1M0.
Under general anaesthesia, a radical laryngectomy with simultaneous tracheostomy and neck lymph node surgery was performed.
From the U-collar neck incision, the neck triangles were exposed after dissection of the platysma neck flap and ligation of the anterior veins, and lymph nodes were dissected on the right group III, II B and IV, on the left group III and conglomerate group IIB.
The sternocleidomastoid and scapulothoracic muscles were dissected from the hyoid attachment, the pyramidal process and thyroid lobes were dissected medially and removed. Bilaterally after dissection, the laryngeal vascular bundles were ligated and transected. After exploration of the trachea, a reinforced endotracheal tube was incised and inserted.
The trachea is severed and removed with the laryngeal tumour from below after bilateral resection of the shaft of the hyoid bone, preserving the tissue margins of the pharyngeal and oesophageal mucosa. After removal of the larynx, the resulting pharyngeal defect is repaired to form the neopharynx. A lingual flap was used to close the pharynx. Sutures were used for the oesophageal and pharyngeal mucosa three-layer closure.
The pharyngeal defect is closed in three layers (mucosal, submucosal and muscularis). This is a traditional three-layer closure [9]. A neck myoplasty and lining to the tongue was performed. The trachea was sewn into the skin producing a tracheostomy. Redon drains were used bilaterally. A tracheoesophageal puncture (TEP) was performed. This allows the insertion of a vocal prosthesis. Creating a connection between the trachea and oesophagus (TEP), is more effective than electrocution or oesophageal speech [10].
Material was collected for histopathological examination. Perioperative and postoperative course without complications. The patient was discharged home in good general condition with recommendations to enrol in voice rehabilitation.
The patient was also referred for voice rehabilitation using a tracheoesophageal voice prosthesis (TEP). As part of the rehabilitation program, he attends regular speech therapy sessions, during which he is trained to properly direct airflow from the lungs into the esophagus to produce sound. Voice restoration with a prosthesis has been shown to allow patients to recover a significant degree of verbal communication ability and overall quality of life after total laryngectomy, with average self reported V RQOL scores indicating substantial improvements in quality of life post rehabilitation. At least 75 % of patients experienced increased quality of life after prosthetic rehabilitation, and outcomes did not appear to be significantly affected by prior radiotherapy or chemotherapy [19].
Studies have also demonstrated that the use of an indwelling voice prosthesis is associated with reductions in symptoms of depression and anxiety alongside improvements in self esteem and psychosocial wellbeing when assessed before and three months after prosthesis placement [20]. Moreover, long term follow up of laryngectomized patients shows that those who achieve successful voice restoration with a TEP generally have satisfactory overall quality of life and functional outcomes; psychological distress remains a key predictor of long term quality of life, underlining the importance of combining speech rehabilitation with psychological support [21].
Speech therapy sessions also focus on teaching control of intonation, articulation, and speech rhythm, which can help maximize prosthesis related vocal outcomes and facilitate social reintegration. This multidisciplinary approach — combining prosthetic voice restoration and dedicated speech pathology support — contributes not only to better communicative function but to enhanced social participation and emotional wellbeing following total laryngectomy.
The total laryngectomy procedure entails the complete excision of the larynx and a segment of the upper trachea, leading to the separation of the respiratory tract and the establishment of a permanent tracheal airway opening in the neck. This intervention prioritizes cancer eradication over the preservation of the patient's phonatory function, as the larynx is a crucial organ for producing natural sound [11].
The loss of phonatory and deglutitory function represents the most formidable obstacles to surmount after laryngectomy, with tracheoesophageal voice prostheses constituting a major breakthrough in postoperative rehabilitation and enhancing patients' quality of life [12]. Despite their benefits, total laryngectomy procedures can give rise to a variety of complications. Notably, the most prevalent postoperative complication is pharyngocutaneous fistula (PCF), which manifests as an anomalous communication between the pharynx and the trachea or skin, resulting in salivary leakage from the pharynx [13].
Vocal rehabilitation represents a critical component of the postoperative convalescence. The concomitant evolution of technology and science has yielded diverse methods and instruments specifically tailored to voice rehabilitation. For instance, the application of tracheoesophageal speech involves the surgical creation of a tracheoesophageal puncture (TEP) and the subsequent insertion of a voice prosthesis [14].
Currently, the tracheoesophageal puncture (TEP) technique represents the preeminent standard in vocal rehabilitation. By utilizing a unidirectional valve, the TEP enables the exhalation of air from the lungs to traverse from the trachea into the oesophagus while preventing the influx of food or fluids in the opposite direction. A voice prosthesis, an assistive device employed after laryngectomy, is situated proximate to the stoma. Through dedicated training, the patient can acquire the skills to channel air from the lungs into the oesophagus, thereby producing vocalizations. Alternately, oesophageal speech necessitates the expulsion of air into the oesophagus, followed by its retrograde motion, culminating in the enunciation of speech sounds. The latter technique requires supervised intervention from a speech therapist [15]. Users of voice rehabilitation techniques report experiencing the best voice quality and overall quality of life when utilizing a voice prosthesis compared to oesophageal speech [18].
In addition to restoring speech, the use of a tracheoesophageal voice prosthesis has been shown to significantly improve psychosocial outcomes. Patients report increased confidence in social interactions, reduced feelings of isolation, and greater participation in professional and family activities. Long term studies indicate that patients who successfully restore their voice with a prosthesis after total laryngectomy achieve satisfactory quality of life and functional outcomes, with a strong correlation between improved voice function and overall quality of life scores, highlighting the importance of psychological wellbeing in post laryngectomy rehabilitation [21].
Regular speech therapy plays a crucial role in maximizing the benefits of prosthetic rehabilitation. Early and continuous speech therapy allows patients to develop effective techniques for managing airflow and articulation, which is associated with higher scores on quality of life assessments such as the Voice Related Quality of Life (V RQOL) and Voice Handicap Index (VHI 10) questionnaires [19]. Moreover, studies have demonstrated that the application of an indwelling voice prosthesis not only enhances voice related quality of life, but also leads to reductions in symptoms of depression and anxiety following rehabilitation, underscoring the broader psychosocial advantages of comprehensive voice restoration programs [20].
Multidisciplinary care involving ENT specialists, speech therapists, and psychological support has been shown to further improve rehabilitation outcomes. Such integrated management helps patients cope with both the functional and emotional challenges after total laryngectomy, facilitating better social reintegration and long term wellbeing [21,19].
Overall, these findings suggest that combining tracheoesophageal prosthesis implantation with dedicated speech therapy and psychosocial support significantly enhances voice quality, participation in social activities, and emotional health, thereby contributing to a more holistic recovery after total laryngectomy.
Within the presented clinical observation, the discussed considerations fully correspond to the actual course of the disease and the selected treatment strategy in this patient. A 66-year-old man with a long history of tobacco use and a diagnosis of laryngeal cancer staged as T3N1M0 underwent radical surgical treatment in the form of total laryngectomy with cervical lymph node dissection, which was consistent with the extent of the tumor process and excluded the possibility of organ preserving therapy. The postoperative course in this patient was uneventful, including the absence of signs of pharyngocutaneous fistula, which is described in the literature as one of the most common complications after total laryngectomy.
During the surgical procedure, a tracheoesophageal puncture was performed to allow subsequent voice prosthetic rehabilitation. This fact directly illustrates the statements presented in the Discussion, according to which tracheoesophageal rehabilitation is considered the primary method of voice restoration after total laryngectomy. In the present case, the tracheoesophageal access was created primarily, which corresponds to the approach described in the literature aimed at early restoration of speech function.
It should be noted that in this clinical observation, objective measures of quality of life, voice function, anxiety, or depression were not assessed using standardized instruments such as V RQOL or VHI 10. The data presented in the Discussion regarding psychosocial effects of voice prosthetic rehabilitation and speech therapy are derived from published studies and are used to contextualize the chosen treatment strategy, rather than representing outcomes obtained directly in this patient.
Nevertheless, referral of the patient for specialized voice rehabilitation with the involvement of a speech therapist after discharge reflects the practical implementation of a multidisciplinary approach described in the Discussion and considered an important component of postoperative management following total laryngectomy. Thus, the presented clinical case illustrates the application of a standard surgical and rehabilitative strategy in locally advanced laryngeal cancer and logically leads to the conclusions formulated in the final section of the article.
In the presented clinical observation, total laryngectomy was performed in a 66-year-old patient with locally advanced laryngeal cancer staged as T3N1M0 as a radical and oncologically justified treatment option in the absence of organ preserving alternatives. The choice of this surgical strategy was determined by the extent of the tumor process and aimed at complete removal of the primary lesion and regional metastatic structures to achieve oncological control. The applied extent of surgery is consistent with literature data indicating high effectiveness of total laryngectomy in advanced stages of laryngeal cancer and is associated with reported five year survival rates ranging from 53 to 86 percent [7,16].
The surgical intervention was followed by an uncomplicated postoperative course, which represents an important immediate outcome of radical treatment. The absence of postoperative complications allowed timely transition to the stage of functional adaptation. As described in the literature, after total laryngectomy the patient required acquisition of alternative mechanisms of breathing and speech [16]. A significant component of the one stage surgical strategy was the performance of a primary tracheoesophageal puncture, which created the anatomical prerequisites for subsequent voice prosthetic rehabilitation.
According to published data, patients after total laryngectomy generally have a higher risk of reduced quality of life and development of anxiety and depressive disorders compared with patients after partial laryngectomy [17]. In the present case, objective assessment of quality of life and psychoemotional status was not performed. However, the patient was referred for specialized speech therapy rehabilitation, which corresponds to accepted postoperative management strategies after radical surgical treatment.
The use of tracheoesophageal voice prosthetic rehabilitation in combination with speech therapy is regarded in the literature as a key factor in restoring verbal communication and improving functional outcomes after total laryngectomy [18,19]. The presented clinical case demonstrates the practical implementation of a comprehensive surgical approach in which radical tumor removal is combined with one stage creation of conditions for subsequent rehabilitation. Thus, management of patients after total laryngectomy should be considered a unified therapeutic process that includes justified radical surgical intervention and planned rehabilitative measures as an integral part of treatment.
Verbal informed consent was obtained from the patient prior to the preparation of this manuscript for the publication of clinical data and any accompanying images.
Ethical approval was not required for this study, as this manuscript describes a single clinical case without any deviation from standard diagnostic or therapeutic procedures. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Wiktoria Janik contributed to the conception and design of the study, coordinated the preparation of the manuscript, and was responsible for drafting the initial version of the text.
Martyna Nowak participated in patient management, data acquisition, and contributed to the interpretation of clinical findings.
Barbara Roguska was involved in data collection, literature review, and supported the drafting of the manuscript.
Katarzyna Szlachetka contributed to the analysis and interpretation of clinical data and assisted in manuscript preparation.
Julia Chołda participated in patient care, data acquisition, and contributed to the critical revision of the manuscript.
Magdalena Matlakiewicz was responsible for data collection, literature analysis, and contributed to manuscript drafting.
Kinga Jamontt participated in the interpretation of clinical findings and provided critical revisions for important intellectual content.
Nina Kubikowska contributed to data acquisition, literature review, and manuscript revision.
Małgorzata Landowska supervised the study, contributed to the conception of the work, critically revised the manuscript for important intellectual content, and approved the final version for publication.
All authors reviewed and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
The authors declare that there is no conflict of interest.

|
||