Erfolgreich durch internationale Zusammenarbeit
Gynecology
Cite as: Archiv EuroMedica. 2026. 16; 2. DOI 10.35630/2026/16/Iss.2.19
Received
18 March 2026;
Accepted 20 April 2026;
Published 27 April
2026
MANAGEMENT AND OBTAINING INFORMED CONSENT COMPLICATED BY INTELLECTUAL DISABILITY IN A PATIENT WITH MRKH SYNDROME - A CASE REPORT
Patrycja
Bździuch¹ 
 ,
Katarzyna Cencelewicz² ,
,
Katarzyna Cencelewicz² ,
Marcelina Podleśna2,3 ,
Joanna Brodowska3,4 ,
Anna Torres⁴
¹
John Paul II Western Hospital, Grodzisk Mazowiecki, Poland;
² 1st
Military Clinical Hospital with the Outpatient Clinic, Lublin,
Poland;
³ Doctoral School, Medical University of Lublin,
Poland;
⁴ Department of Pediatric and Adolescent Gynecology,
Medical University of Lublin, Children's University Hospital, Lublin,
Poland
ABSTRACT
Introduction
The coexistence of Mayer Rokitansky Küster Hauser syndrome and fetal alcohol syndrome in a minor patient with intellectual disability represents a rare clinical and ethical legal situation. Particular complexity arises from the simultaneous presence of two aspects, the clinical justification for surgical intervention in the presence of functioning endometrium within rudimentary uterine structures, and the process of obtaining informed consent taking into account the patient’s cognitive limitations and the involvement of a legal representative. According to a search of the PubMed and Google Scholar databases using keywords related to MRKH, fetal alcohol syndrome, intellectual disability, and informed consent, no publications addressing these aspects jointly were identified.
Aim
To analyze a clinical case of Mayer Rokitansky Küster Hauser syndrome in a patient with fetal alcohol syndrome, with a focus on the justification of surgical management and the specifics of obtaining informed consent.
Methods
A clinical case of a 17-year-old patient with fetal alcohol syndrome, attention deficit hyperactivity disorder, and intellectual disability, evaluated for primary amenorrhea and cyclical lower abdominal pain, is presented. The diagnostic process was based on clinical assessment and imaging methods with karyotype confirmation. Decision making regarding treatment was accompanied by adaptation of communication, assessment of the patient’s decision-making capacity, and the involvement of a legal representative.
Results
Two non-communicating rudimentary uterine horns with signs of functioning endometrium were identified, which caused cyclical pelvic pain and constituted an indication for surgical treatment. Informed consent was obtained from both the patient and her foster mother following step by step explanation of the diagnosis and treatment options. Laparoscopic removal of the rudimentary uterine structures with bilateral salpingectomy was performed. Postoperatively, resolution of pain and improvement in quality of life were observed.
Conclusions
The presented clinical case demonstrates the need for coordinated consideration of clinical indications for surgical treatment in MRKH with functioning rudimentary structures and assessment of a minor patient’s capacity to provide informed consent with the involvement of a legal representative. The case illustrates the clinical rationale for intervention and the decision-making process in the context of intellectual disability.
Keywords: informed consent, intellectual disability, fetal alcohol syndrome, Mayer Rokitansky Küster Hauser syndrome, rudimentary uterine structures, laparoscopic removal.
INTRODUCTION
Prenatal alcohol exposure is an established factor in the development of fetal alcohol spectrum disorders, which are accompanied by cognitive deficit, behavioral disturbances, and a reduced capacity for making informed decisions [1–4]. For the clinical practice of an obstetrician gynecologist, this means a limited ability of the patient to perceive and interpret information about the diagnosis, prognosis, and treatment options, as well as difficulties in weighing the risks and benefits of an intervention. In situations requiring the choice of a surgical strategy, such patients may demonstrate an incomplete understanding of the irreversibility of the intervention, its consequences for reproductive function, and alternative treatment methods, which requires adapted communication and mandatory assessment of their decision-making capacity [5-7].
Mayer Rokitansky Küster Hauser syndrome is a congenital anomaly of Müllerian duct development, characterized by aplasia of the uterus and vagina with preserved ovarian function and a normal karyotype [8-10]. Clinically, the condition presents with primary amenorrhea and anatomical features affecting sexual life [9-12]. In the classical form, pain syndrome is absent [10-11]. Its occurrence is associated with the presence of functioning endometrium in rudimentary uterine structures and impaired outflow of menstrual blood, which leads to the development of cyclic pelvic pain [10-11]. In such cases, the presence of functioning endometrium is a key clinical factor determining the indications for surgical treatment, including removal of the rudimentary structures [10-11].
The combination of a congenital anomaly of the reproductive system and intellectual disability in a minor patient presents particular complexity. In adolescent gynecology, the process of obtaining informed consent includes two mandatory components. The first is the clinical assessment of the patient’s decision-making capacity, which involves evaluation of understanding of information, ability to reason, awareness of consequences, and expression of a stable choice [5-7]. The second is the legal aspect related to the participation of the legal representative, who makes the decision jointly with the patient. In such situations, a balance is required between respect for the patient’s autonomy and the need to protect the patient’s interests [5, 7, 13-14].
According to a search of the PubMed and Google Scholar databases using keywords including Mayer Rokitansky Küster Hauser syndrome, fetal alcohol syndrome, intellectual disability, and informed consent, no publications describing the clinical management of patients with the combination of these conditions were identified. At the same time, the available literature lacks an analysis of the influence of cognitive deficit on the justification of surgical strategy in the presence of functioning rudimentary uterine structures, and no decision-making algorithms have been described that take into account the simultaneous participation of the patient and the legal representative.
The research problem includes two distinct aspects. The first is the clinical justification of surgical intervention in MRKH under conditions of functioning endometrium in rudimentary structures. The second is the process of obtaining informed consent in a minor patient with intellectual disability, taking into account the assessment of the patient’s decision-making capacity and the legal role of the representative.
The aim of the present work is to analyze a clinical case of Mayer Rokitansky Küster Hauser syndrome in a patient with fetal alcohol syndrome, with an emphasis on the justification of surgical strategy.
The scientific novelty of the work lies not only in the description of the combination of the above conditions, but also in the demonstration of the clinical logic of making a decision on surgical treatment in the presence of functioning endometrium in rudimentary structures in a patient with limited decision making capacity, as well as in the analysis of the interaction between the patient and the legal representative in the process of agreeing to the intervention as an element of clinical practice.
The objectives of the study include describing the clinical course of the disease, clarifying the indications for surgical treatment in the presence of functioning rudimentary structures, comparing the chosen strategy with existing clinical approaches to the management of patients with MRKH [10-11], as well as analyzing the process of obtaining informed consent taking into account the patient’s cognitive limitations [5-7, 13-14].
The presented clinical case makes it possible to justify the choice of surgical intervention in MRKH in the presence of functioning endometrium and to demonstrate a practical model of decision making in a minor patient with intellectual disability, including assessment of the capacity to consent and the role of the legal representative.
CASE REPORT
We report the case of a 17-year-old girl with FAS, attention deficit hyperactivity disorder (ADHD) and ID. The patient was born to biological parents with a diagnosed alcohol use disorder, which was associated with adverse effects on fetal development and pregnancy course. The delivery occurred at home and was unassisted, with spontaneous vaginal birth. On the third day of life, the neonate was admitted to the hospital with a low-birth-weight of 2100 grams. Following a two-week hospitalization due to pneumonia, the patient was discharged into foster care.
In March 2024, the patient presented to the gynecology outpatient clinic with complaints of primary amenorrhea and periodic lower abdominal pain. The physical examination revealed sexual maturity at stage V on the Tanner scale. Gynecological assessment showed no abnormalities of the vulva. However, due to the patient’s severe anxiety and lack of cooperation, examination of the vaginal introitus was not feasible. The patient was admitted to the Department of Pediatric and Adolescent Gynecology of the University Children’s Hospital in Lublin for further evaluation. Following informed consent from both the patient and her foster mother, a gynecological examination with transrectal ultrasound was conducted under general anesthesia. The examination revealed a vaginal pouch of about 1,5 cm, a suspected uterine horn, and normally developed ovaries. The ultrasonographic image is presented in Figure 1.
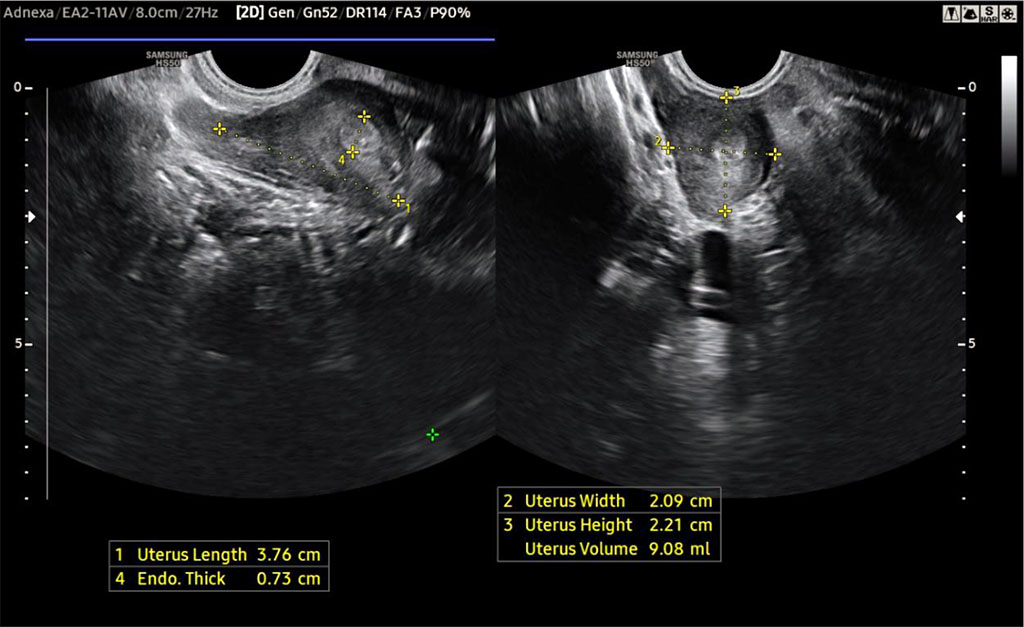
Figure 1. Vestigial uterus visualised on ultrasound
Pelvic magnetic resonance imaging (MRI) demonstrated the absence of the typical anatomy of the uterus, cervix and vagina. Two non-communicating uterine horns with evidence of active endometrium were identified, along with a cystic lesion adjacent to the left uterine horn and non-specific changes in the left ovary. The vaginal wall was visualized only in the lower third of its typical anatomical location, with only a fibrous band observed superiorly.
The results of the laboratory tests were normal. A karyotype test was also performed, confirming a normal 46,XX chromosomal profile.
Based on the diagnostic evaluation, MRKH syndrome was diagnosed. An informative discussion was conducted during which the therapeutic options and prognosis for the patient's future functioning were presented, and all questions were thoroughly addressed. Both the patient and her foster mother expressed full understanding of the current clinical situation. Considering the cyclical pain and lack of reproductive potential associated with the vestigial uterus, a shared decision was made to perform laparoscopic resection.
In May 2024, the patient presented for the surgery. During laparoscopy, peritoneal adhesions, non-communicating uterine horns, a paratubal cyst and stage I endometriosis were identified. The laparoscopic image of the underdeveloped uterus is presented in Figure 2. Additionally, blood-tinged fluid was noted in the rectouterine pouch. The vestigial uterine horns were surgically excised and bilateral salpingectomy was performed. The resected specimens, shown in Figure 3, were submitted for histopathological examination. The patient was discharged several days postoperatively in good general condition.
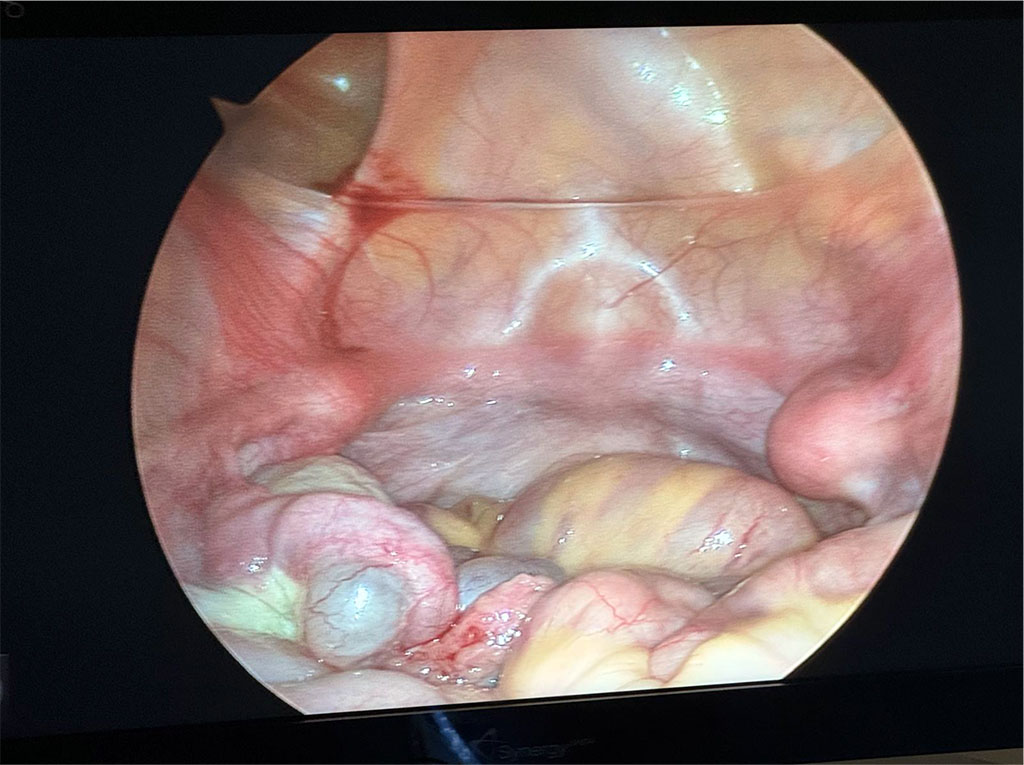
Figure 2. Vestigial uterus visualised by laparoscopy

Figure 3. Laparoscopically removed vestigial uterine horns together with fallopian tubes and paratubal cyst
The case report timeline is presented in Figure 4.
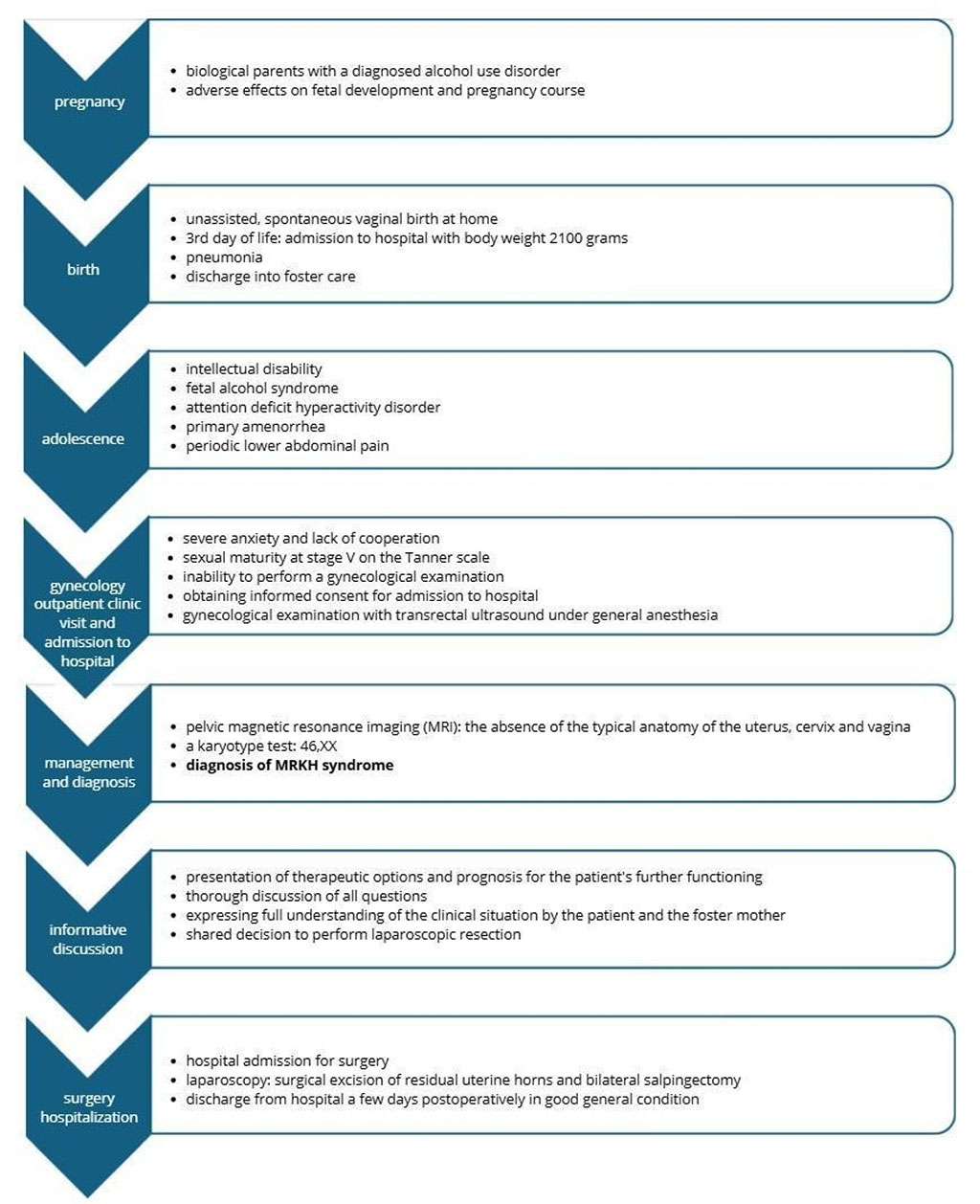
Figure 4. The case report timeline
DISCUSSION
Decision making regarding surgical treatment in young patients with disabilities requires a comprehensive approach that takes into account medical indications, ethical aspects, and respect for patient autonomy [15]. In the present case, the key factor determining the choice of intervention was the presence of functioning endometrium in rudimentary uterine structures, which led to cyclic pelvic pain due to impaired outflow of menstrual blood. Accordingly, the indication for surgery was a clearly defined clinical condition consistent with approaches to the management of patients with MRKH, according to which the presence of symptomatic rudimentary structures with functioning endometrium is considered a direct indication for their removal in order to eliminate pain and prevent further complications [8-11]. It should be emphasized that this case does not involve a classical hysterectomy. The performed intervention consisted of removal of rudimentary uterine structures that do not possess full anatomical or reproductive function. The use of the general term hysterectomy in such situations is incorrect, as it may lead to misinterpretation of the clinical nature of the intervention and its indications.
Patients with intellectual disability should be considered potentially capable of providing informed consent for medical interventions unless proven otherwise [5]. Research indicates that individuals with intellectual disability are generally able to make decisions [6]. However, this ability does not always extend to a full understanding of the potential consequences of their choices. The capacity to provide informed consent improves when information is adapted to the cognitive abilities of the patient [7]. In the present case, the assessment of the patient’s decision making capacity was performed based on key clinical criteria, including understanding of the provided information, ability to reason when discussing treatment options, awareness of the consequences of the intervention, and the ability to express a stable choice. Cognitive limitations required simplification and repeated explanation of information, as well as mandatory involvement of the legal representative. In adolescent practice, this requires a combination of clinical assessment of decision making capacity and the participation of a legal representative as a legally significant part of the process. In the present case, informed consent was obtained from both the 17 year old patient and her foster mother, which is consistent with clinical and legal practice.
The most frequently discussed indications for hysterectomy in women with intellectual disability include elimination of menstruation for hygiene related reasons, prevention of pregnancy in individuals unable to raise a child, and reduction of the caregiving burden on the family [13-14]. However, these indications are predominantly social in nature and differ from the clinical situation presented in this case. Here, the surgical intervention was driven by pain associated with functioning endometrium rather than social factors, which fundamentally distinguishes it from the practices described in the literature.
The available literature does not describe cases that analyze in detail the process of obtaining informed consent in patients with a combination of MRKH and intellectual disability in the context of surgical decision making. At the same time, existing publications on MRKH focus on anatomical and surgical aspects [8-12], including recommendations that intervention is indicated in the presence of symptomatic rudimentary structures, whereas asymptomatic cases may be managed conservatively, while studies on informed consent address cognitive limitations outside a specific gynecological context [5-7]. The present case extends beyond these approaches by demonstrating not only the coexistence of these conditions, but also the need for simultaneous application of clinical criteria for surgical indication and a structured assessment of decision-making capacity in a minor patient with mandatory involvement of a legal representative, forming an integrated clinical, ethical, and legal decision-making framework.
Despite initial difficulties in establishing contact with the patient, the physician’s decision to refrain from performing a gynecological examination at the first visit minimized discomfort and facilitated the development of trust and a therapeutic relationship. The nature of the condition, the rationale for surgical treatment, and its consequences were explained to the patient and her foster mother in a clear and accessible manner. The establishment of a trusting relationship and consistent communication ensured the patient’s participation in the decision making process and enabled informed consent for the removal of rudimentary uterine structures, resulting in the resolution of pain and improvement in quality of life.
The limitations of the present observation include its single case nature, which does not allow for generalizable conclusions and requires caution when extrapolating the findings to a broader patient population. There is no possibility of quantitatively assessing the impact of cognitive impairment on the decision making process and the choice of surgical strategy.
The presented approach may be considered as a model for managing similar clinical situations, but requires further confirmation in a series of observations with a more detailed analysis of clinical and ethical legal aspects.
CONCLUSIONS
In the presented clinical case, obtaining informed consent from a patient with intellectual disability required adaptation of communication and a clinical assessment of her decision-making capacity. The presence of functioning endometrium within rudimentary uterine structures, accompanied by cyclical pelvic pain, determined the choice of surgical management and corresponded to clinical indications for their removal.
The performed procedure consisted of laparoscopic removal of rudimentary uterine structures rather than a classical hysterectomy, which is essential for the correct interpretation of the extent of surgery and its indications. The surgical treatment was determined by clinical, not social, factors.
The scientific novelty of this case lies not only in describing the coexistence of Mayer Rokitansky Küster Hauser syndrome and fetal alcohol syndrome, but also in demonstrating the clinical rationale for surgical intervention in the presence of functioning endometrium combined with the assessment of decision-making capacity in a minor and the involvement of a legal representative.
The available literature does not describe clinical situations in which both the justification of surgical management in MRKH with functioning rudimentary structures and the process of obtaining informed consent in a patient with intellectual disability are addressed simultaneously. The present case fills this gap and demonstrates the integration of clinical and ethical legal aspects of decision making.
Adaptation of communication to the patient’s cognitive abilities, step by step explanation of information, and the establishment of a trusting relationship ensured her participation in the decision-making process and the obtaining of informed consent with the involvement of a legal representative, which allowed surgical treatment to be performed, resulting in the resolution of pain and improvement in quality of life.
A limitation of this report is its single case nature, which does not allow generalization and requires caution in extrapolating the findings.
Thus, the presented clinical case demonstrates an approach to decision making based on the integration of clinical indications for surgical treatment and the assessment of the patient’s capacity to consent, which may be relevant for the management of similar patients in adolescent gynecological practice.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Conflict of Interest
The authors declare no conflict of interest.
Authors' Contributions
Conceptualization and methodology: Patrycja Bździuch, Anna Torres
Literature review and data extraction: Patrycja Bździuch, Katarzyna Cencelewicz, Marcelina Podleśna
Writing – original draft preparation: Patrycja Bździuch, Katarzyna Cencelewicz, Marcelina Podleśna
Writing – review and editing: Joanna Brodowska, Anna Torres
Supervision: Anna Torres
All authors have read and agreed with the published version of the manuscript.
USE OF ARTIFICIAL INTELLIGENCE
The authors would like to acknowledge the use of artificial intelligence tools for language editing and improvement of grammatical accuracy. All content was critically reviewed and supervised by the author to ensure scientific accuracy and logical consistency.
References
- Popova S, Dozet D, Shield K, Rehm J, Burd L. Alcohol’s Impact on the Fetus. Nutrients. 2021;13(10):3452. https://doi.org/10.3390/nu13103452. PMID:34684453.
- Popova S, Charness ME, Burd L, et al. Fetal alcohol spectrum disorders. Nat Rev Dis Primers. 2023;9(1):11. https://doi.org/10.1038/s41572-023-00420-x. PMID: 36823161.
- Riley EP, Infante MA, Warren KR. Fetal alcohol spectrum disorders: an overview. Neuropsychol Rev. 2011;21(2):73–80. https://doi.org/10.1007/s11065-011-9166-x. PMID: 21499711.
- Lange S, Probst C, Gmel G, Rehm J, Burd L, Popova S. Global prevalence of fetal alcohol spectrum disorder among children and youth: a systematic review and meta-analysis. JAMA Pediatr. 2017;171(10):948–956. https://doi.org/10.1001/jamapediatrics.2017.1919. PMID: 28828483.
- Agaronnik N, Pendo E, Lagu T, DeJong C, Perez-Caraballo A, Iezzoni LI. Ensuring the reproductive rights of women with intellectual disability. J Intellect Dev Disabil. 2020;45(4):365–376. https://doi.org/10.3109/13668250.2020.1762383. PMID:35046755.
- Sheerin J, Larkin F, Dockray S. Perceptions of People With Intellectual Disabilities on Autonomy and Decision-Making in Daily Life: A Systematic Review and Synthesis of Qualitative Studies. J Intellect Disabil Res. 2026 Feb;70(3):225–241. https://doi.org/10.1111/jir.70035. PMID:40936314; PMCID:PMC12872376.
- Goldsmith L, Skirton H, Webb C. Informed consent to healthcare interventions in people with learning disabilities — an integrative review. J Adv Nurs. 2008 Dec;64(6):549–563. https://doi.org/10.1111/j.1365-2648.2008.04829.x. PMID:19120568.
- Chen N, Song S, Bao X, Zhu L. Update on Mayer-Rokitansky-Küster-Hauser syndrome. Front Med. 2022 Dec;16(6):859–872. https://doi.org/10.1007/s11684-022-0969-3. PMID:36562950.
- Morcel K, Camborieux L, Guerrier D. Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome. Orphanet J Rare Dis. 2007;2:13. https://doi.org/10.1186/1750-1172-2-13. PMID: 17359527.
- Herlin MK, Petersen MB, Brännström M. Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome: a comprehensive update. Orphanet J Rare Dis. 2020 Aug 20;15(1):214. https://doi.org/10.1186/s13023-020-01491-9. PMID:32819397.
- Matemanosak P, Peeyananjarassri K, Klangsin S, Wattanakumtornkul S, Dhanaworavibul K, Choksuchat C, Getpook C. Clinical features and management of women with Mayer-Rokitansky-Küster-Hauser syndrome in a Thai population. Obstet Gynecol Sci. 2024;67(3):314–322. https://doi.org/10.5468/ogs.23211. PMID:38461809; PMCID:PMC11099089.
- Tsarna E, Eleftheriades A, Eleftheriades M, Kalampokas E, Liakopoulou M-K, Christopoulos P. The impact of Mayer-Rokitansky-Küster-Hauser syndrome on psychology, quality of life, and sexual life of patients: a systematic review. Children (Basel). 2022;9(4):484. https://doi.org/10.3390/children9040484. PMID:35455528; PMCID:PMC9025055.
- Márquez-González H, Valdez-Martínez E, Bedolla M. Clinical, epidemiologic and ethical aspects of hysterectomy in young females with intellectual disability: a multi-centre study of public hospitals in Mexico City. Front Public Health. 2021;9:746399. https://doi.org/10.3389/fpubh.2021.746399. PMID:34869162.
- Márquez-González H, Valdez-Martínez E, Bedolla M. Hysterectomy for the management of menstrual hygiene in women with intellectual disability: a systematic review focusing on standards and ethical considerations for developing countries. Front Public Health. 2018;6:338. https://doi.org/10.3389/fpubh.2018.00338. PMID:30547023.
- Deshpande J. Hysterectomy Dilemmas in Females with Disabilities: A Multidisciplinary Approach. Healthline. 2025;16(2):149–151. https://doi.org/10.51957/Healthline_713_2025.